What is Chronic care management?

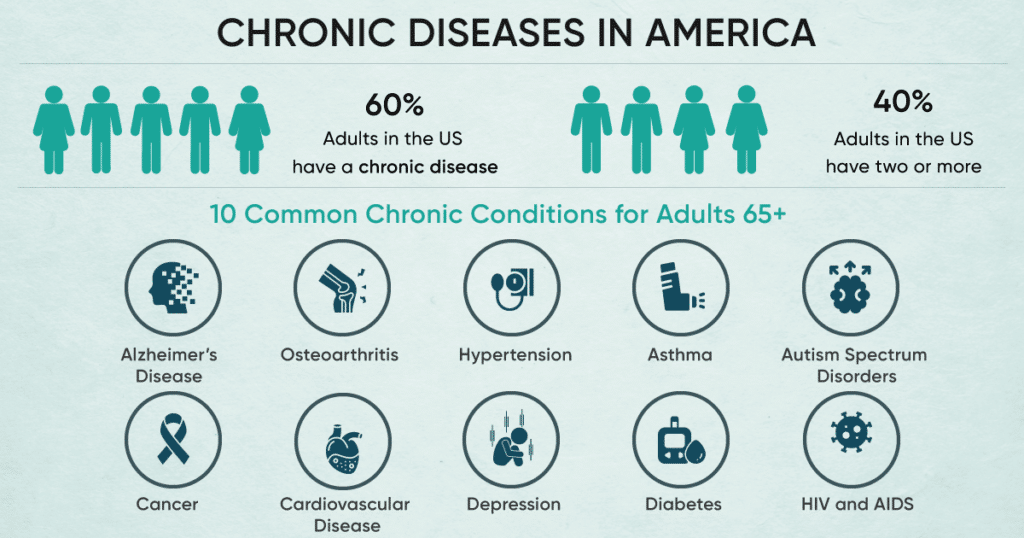
Did you know that over 60% of Americans have at least one chronic disease? Furthermore, 40% of Americans have two or more chronic diseases. Chronic care management (CCM) can decisively assist individuals like these in better well-being for a more extended timeframe.
Receiving chronic care services beyond the doctor’s office allows patients to access multidisciplinary medical support and services. Furthermore, this coordination of services makes it easier for patients to engage with them. It ultimately improves patients’ health while minimizing the costs and slack time associated with visiting multiple clinicians across multiple specialties.
What Is a Chronic Condition?
To begin with, Chronic conditions are diseases or disorders that have been long-term and can not be cured quickly. Also, chronic conditions could cause complications and harm health if you have multiple chronic conditions with rapidly increasing severity. In general Chronic conditions mainly occur in senior citizens above the age of 50 years.
You need at least two chronic conditions from the last six months to avail of CCM services. Following are some primary chronic conditions:
- Alzheimer’s disease
- Osteoarthritis
- Rheumatoid arthritis
- Asthma
- Autism spectrum disorders
- Cancer
- Cardiovascular disease
- Depression
- Diabetes
- HIV and AIDS
What is Chronic Care Management?
Generally, chronic care management (CCM) is a healthcare service focusing on helping patients manage their chronic conditions effectively. In addition, chronic care management services are covered by Medicare Part B, and CMS offers reimbursement for the same.
The Centers for Medicare & Medicaid Services (CMS) have endorsed this service. Their goal is to improve patient outcomes and chronic disease management. Home health services will be offered to patients, leading to better outcomes.
Introducing CCM services not only aims to identify future risks and provide remote health services to patients but also reduce health costs. Also, CCM providers can bill monthly services by submitting claims to Medicare and getting reimbursement.
CCM services offer many benefits. One of the best is 24/7 remote monitoring. Healthcare providers are always available in case of an emergency.
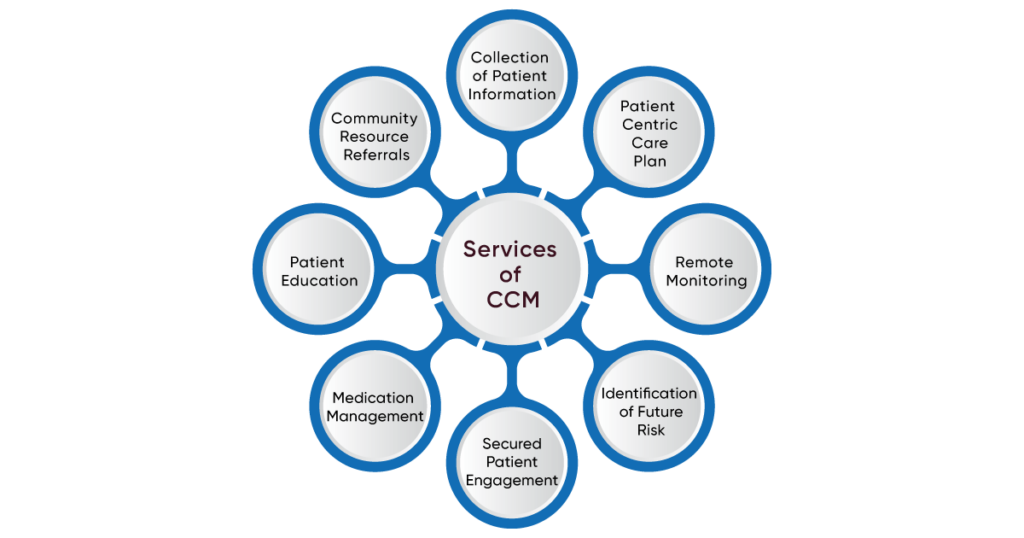
Apart from this, CCM has other essential services as below:
1. Gathering of patient clinical and financial data in a structured way
- Collection of patient information
2. Creating a comprehensive electronic care plan for each patient
- Patient-centric care plan
3. Managing remote patient services and transition
- Remote monitoring
4. Coordinating with other providers and sharing medical records securely
5. Providing continuous care coordination and tracking patient record
6. The focus of preventive care results in less future health risk
- Identification of future risk
7. Improving patient engagement through messaging, video calls, and real-time updates.
- Secured patient engagement
8. Coordinating information and referrals between your entire medical team
9. Refilling prescriptions
- Medication management
10. Patient health education
- Patient Education
11. Community resource referrals
Chronic care management particularly involves a team of healthcare professionals who work together to provide comprehensive care for patients with chronic conditions. This team may include doctors, nurses, care coordinators, and other healthcare professionals. Furthermore, CCM aims to help patients manage their conditions, improve their quality of life, and reduce healthcare costs.
A care plan tailored to patients’ needs is crucial to chronic care management. This plan then ensures that the patient’s needs are met. This plan may include various services, such as regular checkups, medication management, and lifestyle counseling. Care coordinators may also help patients navigate the healthcare system, schedule appointments, and ensure they receive appropriate care.
Another essential aspect of chronic care management is communication. Healthcare professionals must work together in order to ensure that patients are receiving the care they need and are monitoring their conditions effectively. It may also involve sharing information about medication changes, test results, and other essential updates.
In addition to improving patient outcomes, chronic care management can help reduce healthcare costs. By providing ongoing care and monitoring, healthcare professionals can help prevent complications that may lead to hospitalizations or emergency room visits. It can ultimately save patients and healthcare systems money in the long run.
Various factors, such as genetics, lifestyle choices, and environmental factors, can cause chronic conditions. However, healthy life choices can prevent or manage Chronic conditions. These include keeping a healthy weight, exercising regularly, and avoiding smoking and drinking too much alcohol.
Treatment for chronic conditions often involves a combination of medication, lifestyle changes, and other interventions. Thus, individuals with chronic conditions must work closely with their healthcare providers to manage them effectively and prevent complications.
Living with a chronic condition can be challenging, but leading a fulfilling life with the proper support and management is possible. Stay informed about your condition. Take an active role in your healthcare. Seek support from friends, family, and healthcare providers when needed.
Who can provide Chronic Care management services?
We all know that Medicare requires a qualified healthcare provider (QHP) to provide reimbursement for CCM services. Whereas non-healthcare providers cannot bill for CCM services.
As per the CMS guidelines, CCM services can be provided by the following :
- Physician
- Clinical nurse specialist (CNS)
- Nurse practitioner (NP)
- Physician Assistant
- Certified nurse-midwife
States may impose a unique set of rules on who may and cannot apply for Medicare services. They are not necessarily the same as Medicare standards.
What Is an Initial Visit?
An initial visit for chronic care management is essential to manage chronic conditions. CCM services begin after the completion of the initial visit. This visit can in either case be in person or a face-to-face visit.
During this visit, the healthcare provider will gather important information about the patient’s medical history, health status, and treatment plan. This information will then help the healthcare provider create a personalized care plan for the patient.
Initial visits include annual wellness visits, transitional care visits, or pre-scheduled routine checkups. Providers cannot bill initial visit charges under the CCM program. CMS does not pay for this. Initial visits may include annual wellness visits, transitional care visits, or pre-scheduled routine checkups. Providers cannot bill for initial visit charges under the CCM program.
How do Chronic care management services work?
Chronic care management services involve some significant steps by which patients can access care from providers under the CCM program. Please continue reading the below steps of CCM.
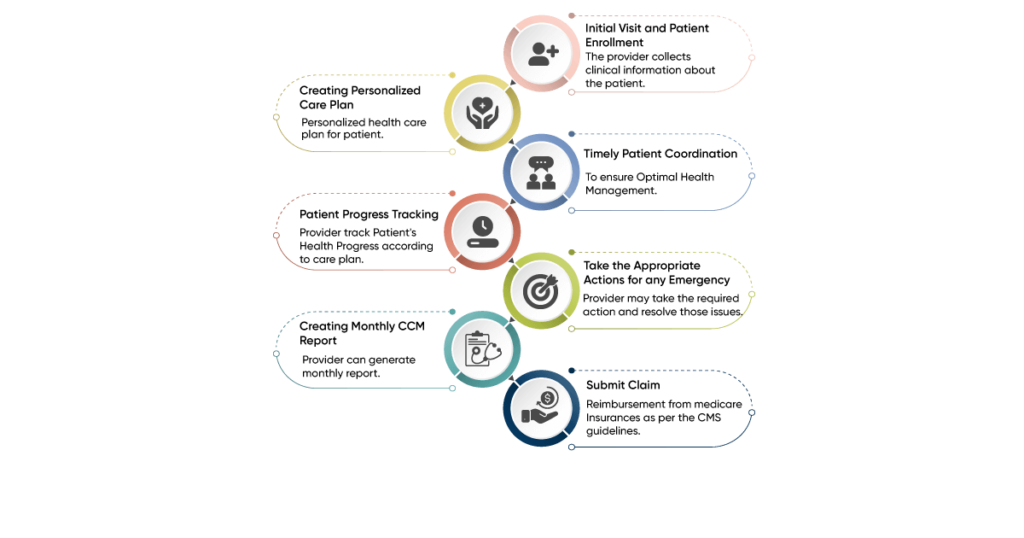
Initial visit and patient enrollment
The initial visit is the very first step of CCM services. The provider collects clinical information about the patient, including their chronic condition, severity, and onset date. Based on this information, the provider determines if the patient is eligible for CCM services. If the patient is eligible, the provider can get their consent and enroll them in CCM services.
Creating a personalized care plan
The patient is enrolled in CCM services. The provider creates a personalized health care plan for them. This care plan is intended to assist patients with chronic illnesses in managing their conditions. The plan includes the following:
- Goals to be achieved to control chronic diseases
- Potential barriers to following the plan
- Symptoms to reduce
- Interventions that may be necessary
- Medication and allergies (if applicable)
- A support team to coordinate with the patient.
Communicating with patients to evaluate patient health- Timely patient coordination
Providers must maintain consistent communication with their patients to ensure optimal health management. This can be done through phone calls, video conferences, audio calls, and two-way messaging. This enables timely updates to the patient’s health information. It also allows reviewing information logged through the patient’s mobile app.
Determine the patient’s progress and update the care plan- Patient progress tracking
Providers can analyze patient information collected in the system to determine the patient’s health progress. They can then mark the progress and modify the care plan if necessary.
Take the appropriate actions for any emergency.
The provider may take the necessary action and resolve those issues if he finds any uncertainty closer to the patient’s health
Creating monthly CCM report
After completing the month of CCM services, the provider can generate a monthly report for each patient. This report primarily includes:
- Patient information
- Enrollment details and consent
- The care manager and care team associated
- Clinical details
- Care plan progress and updates
- Vital readings, if applicable
- Time logged by physician and care team.
Submit a claim for monthly RPM service provided
Providers can submit the claim for monthly RPM services. They can get reimbursement from Medicare insurance as per the CMS guidelines. They must submit monthly reports to insurance companies to get maximum reimbursement.
What Does a Comprehensive Care Plan Include?
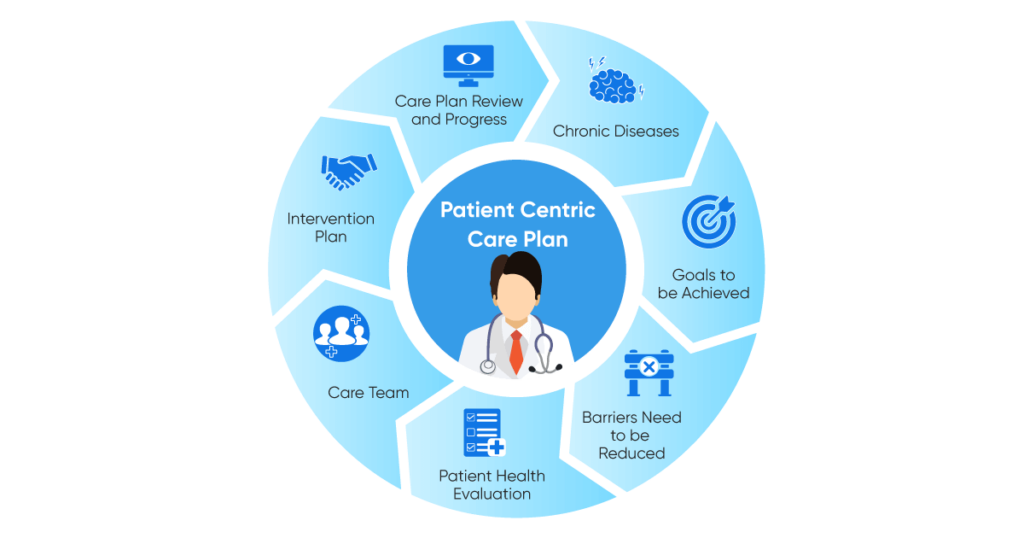
A comprehensive care plan is a detailed healthcare approach to meet a patient’s needs. The patient’s care is based on their medical history, current health status, personal preferences, and other relevant factors.
A comprehensive care plan typically includes several components depending on the patient’s needs and healthcare setting.
Some of the critical components of a comprehensive care plan are:
- Chronic diseases: Providers must consider a patient’s chronic diseases when creating a care plan. This should include the severity of the disease, potential health effects, and any associated symptoms. Desired care should also be taken into account.
- Goals to be achieved: The provider can create a care plan which is basically goal-oriented. Care providers should set trackable and non-trackable goals to manage patient care better. This can help patients improve their health outcomes.
- Barriers need to be reduced: There may be barriers that prevent patient growth. So these barriers must be identified and removed to achieve patient health outcomes.
- The treatment plan should include evaluating the patient’s medical history, health status, and personal preferences. This will then ensure a comprehensive care plan. It may include medications, therapies, lifestyle changes, or other interventions.
- Care team: A comprehensive care plan should not only identify the healthcare providers involved in the patient’s care but also their roles and responsibilities. It may include primary care physicians, specialists, nurses, and other healthcare professionals.
- Create an intervention plan: This plan should include a communication strategy. Also, this strategy should detail the patient’s condition, treatment course, and any changes to their care. Share this strategy with everyone involved in the patient’s health care plan. It may include regular meetings, phone calls, or electronic communication.
- Follow-up and monitoring: This will help to ensure the patient’s care is effective and any issues are resolved quickly. It may include regular check-ins, diagnostic tests, or other assessments
Will You Have to Pay For Chronic Care Management?
Chronic care management (CCM) is a Medicare-billable service designed to enhance the lives of both patients and clinicians.
You are eligible for CCM treatments if you have Medicare and two or more chronic diseases. However, the symptoms must continue anywhere from 12 months to the remainder of your life to be eligible.
The purpose of CCM services is to provide coverage for non-face-to-face encounters. Moreover, these encounters are needed to manage multiple chronic illnesses effectively.
Since chronic care management services are a Medicare Part B benefit, only 80% of these services are covered by Medicare. You’re then responsible for 20 percent of the total CCM bill.
People with Medigap or covered by Medicare and Medicaid will likely not have to pay a copay. Instead, your medical team should charge 20 percent to the agency that provides your added coverage.
What Are the Chronic Care Management Codes?
Chronic care management (CCM) codes are used in healthcare. They are billing codes that reimburse providers for ongoing care of patients with chronic conditions. The Centers for Medicare and Medicaid Services (CMS) introduced codes in 2015. Furthermore, these codes encouraged and helped provide ongoing care for patients with multiple chronic conditions.
There are several CCM codes that providers can use to bill for services related to chronic care management, including:
- CPT code 99490: Covers initial 20 minutes of non-face-to-face clinical staff time per calendar month. This time is directed by a physician or other qualified healthcare professional (QHP).
- CPT code 99439: Covers an additional 20 minutes of non-face-to-face clinical staff time per calendar month. This time is directed by a physician or other qualified healthcare professional (QHP).
- CPT code 99491: Covers at least 30 minutes or more of clinical staff time each calendar month. A physician or other qualified healthcare professional directs this time.
- CPT code 99437: Covers 30 extra minutes of clinical staff time per month. A physician or other qualified health professional must direct this staff time.
- CPT code 99487: Covers complex chronic care management services. These services are particularly for patients with significant chronic conditions. Moreover, these conditions require a high medical evaluation, management, and coordination.
- CPT code 99489: For patients given 20 minutes or more of care in one month, CPT code 99489 provides an extra 30 minutes of care by a healthcare professional.
Healthcare providers can be reimbursed using codes to care for patients with chronic conditions. This includes coordinating care between various healthcare providers, reviewing medication regimens, and creating care plans. Furthermore, CCM codes can improve the quality of care for patients with chronic conditions. This can then reduce healthcare costs by minimizing hospital readmissions and other adverse events.
What Is the Difference Between Principal and Chronic Care Management?
The main difference between Principal and Chronic Care Management is the number of chronic conditions being managed. PCM focuses on a single high-risk condition, while CCM focuses on patients with multiple chronic conditions. Another significant difference is the level of care coordination involved. Comparatively, CCM requires more extensive care coordination between the care team, the patient, and other specialists involved in the patient’s care.
Chronic Care Management Software Features
1. Seamless onboarding with an initial interview:
Thinkitive’s CCM software solutions enable healthcare providers to seamlessly onboard patients. This includes managing patient information, such as medical history, medications, and treatment plans. An initial interview is also part of the process.
2. Manage & track care in line with the care plan:
Our software assists healthcare providers in coordinating care between multiple providers and specialists. Also, providers can track patient progress according to the care plan assigned.
3. Customizable personalized care plans for each patient:
Thinkitive’s CCM software provides tools to create and manage customizable, personalized care plans. Each plan is tailored to the individual patient accordingly. Moreover, these plans are specific to each patient’s medical needs and goals.
4. Remote Monitoring:
Remote monitoring is supported by the software. This furthermore allows healthcare providers to track patients’ vital signs and other real-time health data. This monitoring then helps healthcare providers ensure the best possible patient care.
5. Real-time alerts and notifications:
Real-time alerts and notifications provide updates on patient health. They also provide information on tasks that providers have to complete.
6. Secure Patient Engagement using calls and messaging:
The software includes features to engage patients in their care. Examples of healthcare services include educational materials, medication reminders, and communication tools. These tools can also be used to contact patients via phone, messaging, and video calls. These tools allow patients to stay connected with their care team.
7. Get paid for non-face-to-face services more efficiently:
Thinkitive’s CCM software solutions can help. Healthcare providers can then use them to track and document CCM services. It also supports billing for Medicare reimbursement.
8. Informative patient population dashboard with insights:
The software offers analytics and reporting capabilities to help healthcare providers evaluate the success of their CCM programs. It also provides a patient population dashboard with insights. It also helps identify improvement areas and demonstrate their value to patients and payers. This is achievable through an informative patient population dashboard with insights.
Conclusion
In conclusion, chronic care management (CCM) is a vital healthcare service that offers a lifeline to the growing number of Americans with chronic conditions. It undoubtedly extends care beyond the doctor’s office, providing patients with comprehensive support and coordination of services. CCM not only improves patient health and engagement but also reduces healthcare costs associated with multiple specialist visits. Thus, with qualified healthcare providers, personalized care plans, and CCM codes and software, we can enhance the quality of life for those managing chronic conditions and ensure a healthier future for all.




