Implementing HL7 Interfaces for EHR Integration

Today, with modern healthcare becoming fast, even if a single report is delayed or reaches systems in the wrong format, patient care suffers greatly. This is where having connected systems that can exchange data seamlessly becomes important. And for that, EHR integration is the key.
Moreover, in this information-driven modern healthcare, having quick access to complete patient data is crucial. HL7 (Health Level 7) interfaces make this possible by connecting all the digital devices from wearables and medical devices to labs and pharmacies under one system.
So, whether it’s a sudden increase in heart rate or high blood sugar, everything is automatically updated in your EHR. However, it not only gets updated but also stored in the language the system understands, meaning you get a translator that is active 24/7.
And this is what makes the HL7 standard more popular, along with its simplicity and ease of implementation. Because of this, even with new and advanced standards like FHIR (Fast Healthcare Interoperability Resources), HL7 interfaces still remain widely adopted in all legacy systems. You can easily implement this if you plan well and choose the right EHR integration services.
In this blog, we will explore how HL7 interfaces work, pre-implementation planning, tech architecture, and how it integrates with different EHRs.
So, let’s get started and see how these interfaces bring EHR interoperability!
Understanding HL7 Standards: The Foundation of Healthcare Data Exchange
HL7 has remained the backbone of healthcare interoperability since its creation in the 1980s. However, it has changed since then, and even with the new standards like FHIR emerging, it’s still the most adopted standard. Let’s take a look at how it changed and other parts of HL7.
- HL7 Version Evolution & Selections
HL7 was founded in 1980, and since then, it has evolved. HL7 v2.x released in 1987, was adopted quickly and widely, and still, 95% of the systems use this version of HL7. Although there were later versions, such as HL7 v3, it was not adopted well because of its complexity in implementation. The reason was the XML format that was richer in semantics but too complex. So, when it comes to deciding between the two, it completely depends on your infrastructure, vendor capabilities, and migration costs for legacy systems.
- Core HL7 Message Types & Structures
HL7 has four core messaging formats that work with different interfaces like EHRs, labs, pharmacies, and billing systems. Here are the formats:
- ADT (Admission, Discharge, Transfer): This format is used to exchange and track patient demographic data from system to system.
- ORM/ORU (Order & Result): This is used to manage, order, and share details of lab tests, procedures, and their results.
- MDM (Medical Document Management): Handles clinical documents and reports.
- DFT (Detailed Financial Transactions): This format is for exchanging data from billing and financial systems.
- HL7 vs FHIR: Choosing the Right Standard
If your system is established and has a mature infrastructure, then using HL7 is the right choice. However, in the case of modern systems that require flexibility, FHIR is the right choice as it has API-based integration. Many organizations usually go with a hybrid model that balances old legacy systems while connecting newer systems, such as mobile and web-based integration. Cost, complexity, and future-proofing are also the deciding factors.
- Industry-specific HL7 Requirements
Every system or organization works with a different HL7 format, and its requirements change. For instance, hospitals need ADT and DFT for tracking patient data and exchanging billing information. Whereas ORM/ORU is used by labs, pharmacies require prescription-focused interfaces. So, with each service or organization, the HL7 requirements become different.
Get our HL7 Message Type Reference Guide with Implementation Examples for Easier Implementation
Download nowPre-Implementation Planning: Setting Up for HL7 Success
Better planning of the implementation can save you from many troubles ahead and can make implementing HL7 interfaces much easier. Moreover, most implementations that fail have either not been prepared well or have not decided on countermeasures beforehand. So, let’s see how you can plan better before even starting the implementation.
- Technical Assessment & Gap Analysis: This is the first step towards a seamless integration. When you implement HL7, you need to understand what your system needs to work properly with these interfaces. Moreover, for data to flow smoothly and securely, you need to assess your data mapping, network security, and identify gaps and requirements.
- Stakeholder Alignment & Requirements: The ones using the systems know what it lacks and what they need to solve their issues, so connecting with the stakeholders and aligning the goals with their needs gives you a more accurate and better implementation plan and clarifies your organization’s needs. Also, conducting workflow analysis tells you how messages should flow between systems. Allocating resources based on skill and coordinating with Epic and Cerner vendors helps in making quick and right decisions. Identifying your compliance and regulatory gaps makes it easier to plan for the implementation needs.
- Architecture Design Decisions: If you want the system to function seamlessly, the right architecture is the key. So, choosing between the point-to-point connections or the interface engine for scaling needs to be decided beforehand. Another decision that you need to make is deciding between real-time data exchange and batch processing, but going with a hybrid approach can be beneficial. Designing error-handling protocols and planning retry mechanisms is also important for better efficiency and accuracy.
- Project Scoping & Timeline Development: Define a phased rollout with clear milestones. Establish a robust testing environment, outline go-live strategies with rollback contingencies, and allocate resources across each stage.
If you plan all of this pre-implementation, then you can reduce the risks of integration significantly, giving a more robust foundation for a successful HL7 deployment.
Technical Implementation: Building Robust HL7 Interfaces
Without a robust foundation, even a well-coded HL7 interface can crumble and struggle to exchange information seamlessly. That’s why an EHR integration with an HL7 interface needs to be paired with an architecture that can hold it all together without compromising its efficiency.
So, to make developing an interface easier, we have created some best practices. You need to properly parse and validate all messages, map segments, and fields accurately, and implement custom Z-segments when EMR-specific data is needed. Including this while developing the platform makes data flow smoother.
Connection methods and protocols form the backbone of reliable integration. Most HL7 interfaces use MLLP over TCP/IP, often secured with VPNs or other encrypted connections. Depending on workflow needs, integrations can be real-time or batch-based. Choosing the right approach balances system performance, message volume, and operational requirements.
Data transformation and mapping are critical for interoperability. Field-level mapping ensures that ICD-10, CPT, and LOINC codes are translated correctly, units are standardized, and optional or missing fields are handled gracefully. The table below summarizes key mapping considerations:
| Mapping Area | Example | Notes |
| ICD-10 Codes | EHR A → EHR B | Ensure code versions match |
| LOINC Codes | Lab results | Standardize units & formatting |
| Optional Fields | Allergy notes | Provide defaults for missing data |
Finally, error handling and logging are essential. Implement ACK/NACK messaging, maintain error queues for retries, and set up comprehensive logging and alerts. These strategies help catch issues early, simplify troubleshooting, and ensure reliable HL7 communication across systems.
Access our HL7 Implementation Toolkit with Code Samples & Templates
Download nowIntegration with Major EHR Systems: Platform-Specific Considerations
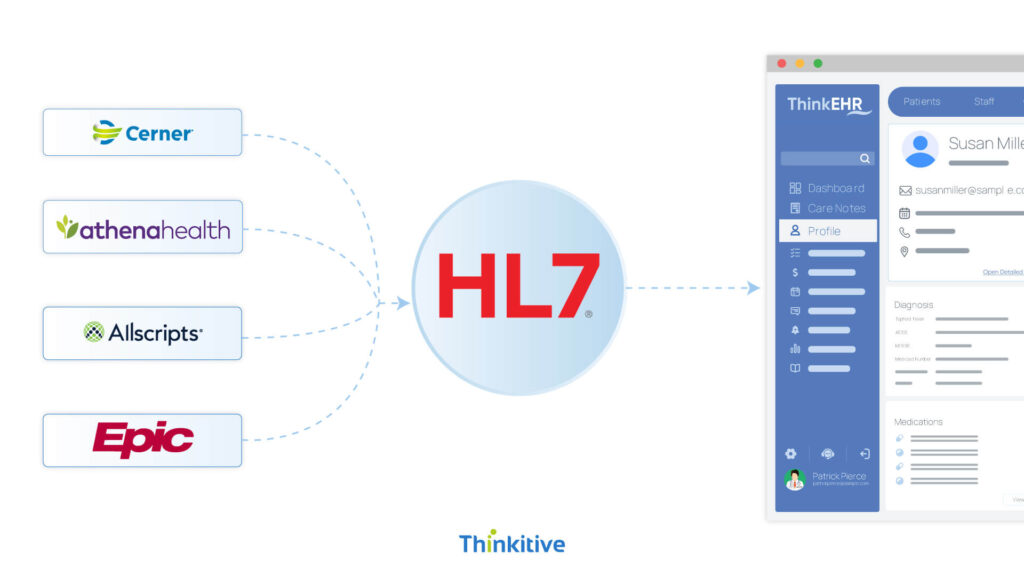
Every EHR is different, and so are the requirements for its integration with HL7. So, you need to understand what each system needs to integrate correctly. Even the standards differ, interface engines change, and knowing this early reduces errors and ensures seamless integration.
- Epic EHR Integration via HL7: To integrate Epic, HL7 uses the Bridges interface engine for routing messages to their right place, and for storing data, it uses the Chronicle database, which requires careful planning. It also supports custom message formats and extensions. Most of the testing happens in Epic’s playground environment, giving greater accuracy before deploying for production.
- Cerner Integration Requirements: This EHR integration uses Open Engine architecture along with the variations from its Millennium platform. Custom Cerner message types are often needed to integrate with PowerChart and other clinical modules.
- Other Major Platform Integrations: Other EHR platforms, including Allscripts, Athenehealth, NextGen Healthcare, and eClinicalWorks, also have specific integration requirements. Allscripts provides services to Sunrise Clinical Manager, whereas Athenahealth uses APIs to connect endpoints. Like this, every other integration comes with specific requirements; you need to understand those before proceeding with HL7 integration.
- Legacy System Challenges: Legacy systems like MEDITECH present additional challenges, often using non-standard HL7 formats or proprietary message structures. Character encoding issues and performance limitations are common, requiring careful optimization to handle high message volumes.
Understanding these platform-specific requirements allows healthcare organizations to design HL7 interfaces that are reliable, scalable, and compatible across diverse systems, minimizing errors and improving patient care.
Testing, Validation, & Quality Assurance
Only developing and deploying the integration is not enough; you need to make sure that it works as intended and the quality is what you were promised. That’s where testing, validation, and quality assurance come in.
- Comprehensive Testing Strategy: Developing a testing plan that includes all points is necessary for HL7 interface implementation to be efficient. For that, unit testing ensures each message type is formatted and transmitted correctly, while integration testing verifies smooth data flow across systems. Volume and stress testing evaluate performance under high message loads, and end-to-end workflow validation confirms that clinical processes function seamlessly with the integrated data.
- Message Validation Technique: Maintaining data integrity requires validation. HL7 structure validation tools check message syntax, while field-level rules ensure accurate and complete data. Business logic rules ensure accurate and complete data. Business logic validation confirms messages behave as expected within clinical settings and workflows. Compliance checks guarantee adherence to HIPAA and other regulatory standards.
- Clinical Safety Testing: Patient safety is paramount. Testing must verify patient matching and identification accuracy, confirm handling of critical lab values, and ensure allergy and medication alerts are reliably transmitted. Additionally, order and result integrity checks confirm that clinicians receive accurate, actionable information.
- Performance Optimization: High-performing HL7 interfaces require careful tuning. Message throughput benchmarking, queue management, database query optimization, and network latency minimization are essential to maintain speed and reliability, especially in high-volume environments.
Conclusion
In a nutshell, modern healthcare needs a connected ecosystem to provide seamless and continuous care. And here HL7 becomes the bridge to connect these systems. HL7 interfaces help hospitals and clinicians exchange data swiftly and provide instant access to all patient data.
So, the HL7 interface implementation is a crucial step for every healthcare organization. You need to carefully plan, understand, and execute the whole process. Everything from customizations, gaps, and technology architecture plays an important role in making this implementation a success.
Click here to book your assessment call and take your first step towards more connected healthcare with HL7 interfaces.
Frequently Asked Questions
The main difference between HL7 v2 and v3 is the complexity of implementation. HL7 v2 is more widely adopted, lightweight, and flexible, making it easier to implement. HL7 v3, while more robust in message format using XML, is highly complex. Based on practicality, most organizations prefer v2 over v3.
A HL7 interface implementation can take between a few weeks and a few months, depending on complexity, need for system infrastructure, vendor cooperation, and testing requirements. Simple, single-feed interfaces may go live in four to six weeks, while larger multi-system integration can stretch closer to three to four months for full rollout.
You can build point-to-point HL7 connections, but they get messy fast as the number of systems grows. An interface engine simplifies things by acting as a central hub, making integrations easier to manage, scale, and maintain while reducing long-term costs and technical headaches.
The biggest hurdles are inconsistent standards, legacy system limitations, and poor documentation. Add in mismatched data formats, and you’ll have integration headaches. It’s less about HL7 being flawed and more about how each vendor interprets and implements it differently. Alignment and testing are everything.
Depending on complexity, custom requirements, and vendor involvement, HL7 interface costs can range from $10,000 to $30,000+ per interface. It’s not just about development; factor in ongoing maintenance, testing, and upgrades. The real value comes when interfaces reduce manual work and costly data errors.
Yes, HL7 is designed for near real-time exchange of patient data like labs, orders, and results. The catch is how the interface is implemented. If systems aren’t optimized, you’ll face delays or errors. Done right, HL7 can move critical updates almost instantly between systems.
Testing isn’t optional. Teams typically validate message structures, check field-level accuracy, and run end-to-end workflow simulations. Volume and stress testing ensure stability under load. The goal is to catch mismatches or drop data early so that providers don’t have to deal with broken results in live care.
HL7 (v2) is the older, widely used messaging standard, great for legacy workflows. FHIR is modern, API-driven, and web-friendly, perfect for mobile apps and cloud systems. Think of HL7 as faxing structured data, while FHIR is like secure, real-time web calls. Both often coexist in healthcare.
Errors happen, such as missing fields, invalid codes, or misrouted messages. The best practice is to log everything, send acknowledgment messages, and set up alerts for failures. Automated retries plus manual review for persistent errors keep data flowing without compromising patient safety or compliance.
Yes, but it’s rarely plug-and-play. Most organizations layer FHIR APIs or upgrade middleware rather than replacing v2 outright. Hybrid models are common: v2 still handles legacy exchanges, while FHIR supports modern apps. The trick is mapping messages cleanly across standards without losing critical data.
Since HL7 doesn’t enforce security, organizations must add safeguards like TLS encryption, VPN tunnels, and strong authentication. Role-based access and audit logs are essential, too. Think of HL7 as the language and security as the lockbox—protecting the messages is up to you.
Compliance comes down to securing PHI in transit and at rest. That means encryption, access controls, audit trails, and strict data-sharing policies. Regular risk assessments and vendor agreements (BAAs) are also a must. In short, HL7 is just the plumbing; compliance depends on how you secure the pipeline.




