EHR Integration Standards: From HL7 to FHIR & Beyond
While interacting with one of our clients, the problem of data silos has been very persistent across the healthcare IT landscape. Many providers, in fact, suggested this as one of the major barriers to providing holistic care.
Believe it or not, but during a conversation with a practice owner, they had held their value-based care model for a year because the data they wanted was connected with their system.
This was when I hit the internet to find if it had been a universal problem. That is when I came across this study by IBM, which stated that siloed data had hindered 77% of healthcare organizations’ ability to perform real-time analytics and make timely data-driven decisions.
Upon digging deeper into this problem, some unsettling facts did create uneasiness about the future of healthcare. You see, despite producing 30% of the total data, almost 80% to 90% of all healthcare data is still unstructured, according to Fast Data Science.
The impact? Healthcare providers spend 30-40% of their working hours on data management, administrative tasks, and other clerical work such as documentation in EHRs.
This clearly showed why healthcare practices have been actively seeking EHR integration projects. But the solution to these problems was far from that. It was hidden in the intricacies of that, or how the data was stored.
You see, EHR integration standards can be the solution to eliminate data silos in healthcare and will be the first step in building a truly connected healthcare ecosystem.
As a healthcare practice, you need to move beyond system connections and rely on meaningful data exchange. And for this, healthcare interoperability standards are something that makes it happen.
On that note, let’s discuss what EHR integration standards are and how they set the foundation of a scalable and compliant healthcare system.
So, without further ado, let’s get started!
Which EHR Integration Standards Should You Choose? –
Get Free Consultation
The Foundation: Semantic & Healthcare Data Standards
Before moving further ahead, tell me why you think standardized clinical meaning matters?
You see, with a connection, two systems can successfully exchange data with each other, and the HL7 international standards help them in that. However, they are not semantically aligned. Meaning, the meaning of the data remains inconsistent across the system, and it does not have any context.
Due to this, the diagnosis can be interpreted differently, lab values may differ across care teams, and errors in mediations can increase. This further leads to clinical ambiguity, errors, and poor decision-making.
Core Healthcare Terminology Standards
This is where healthcare terminology standards come into play. These standards form the backbone of semantic interoperability. Here are a few standards that you should know:
- SNOMED CT (Clinical Terminology): It is a comprehensive clinical vocabulary for conditions, symptoms, and procedures. Furthermore, it enables granular and precise clinical documentation.
- LOINC (Labs & Observations): These standard terminologies are used for lab tests and clinical measurements. With these standards, you can ensure that the lab results are consistently identified across systems.
- RxNorm (Medications): These standards normalize drug names across brands, generics, and dosage forms. It has been critical for ePrescriptions and medication reconciliation.
- ICD (Diagnosis Coding): These standard codes are specific diagnosis codes used worldwide for billing and reporting. It provides a standardized diagnosis classification and has become essential for administrative interoperability.
How Consistent Vocabularies Improve Interoperability?
When you use standardized terminologies, data becomes comparable across systems and organizations. This allows clinical decision support tools to interpret inputs accurately, and analytics become reliable and scalable.
Furthermore, with AI models, the process can be streamlined and made faster with clean, structured, and labeled data.
Role of Terminology Services & Value Sets
Now, to make use of these standards, modern systems have been relying on terminology services. These services map local codes to standardize vocabularies, validate code systems (SNOMED, LOINC, etc), manage value sets, and enable real-time lookups via APIs. This reduces variations in data entry, improves data quality at the source, and simplifies downstream integration.
AI-Assisted Normalization of Clinical Data
The introduction of AI can solve the problem of unstructured data. You see, with AI and NLP, you can extract entities from clinical notes and map free text into standardized codes. Along with that, it can also be used to detect duplicates and inconsistencies in data.
With AI, you can reduce manual coding efforts, improve semantic consistency at scale, and enable advanced analytics and AI applications.
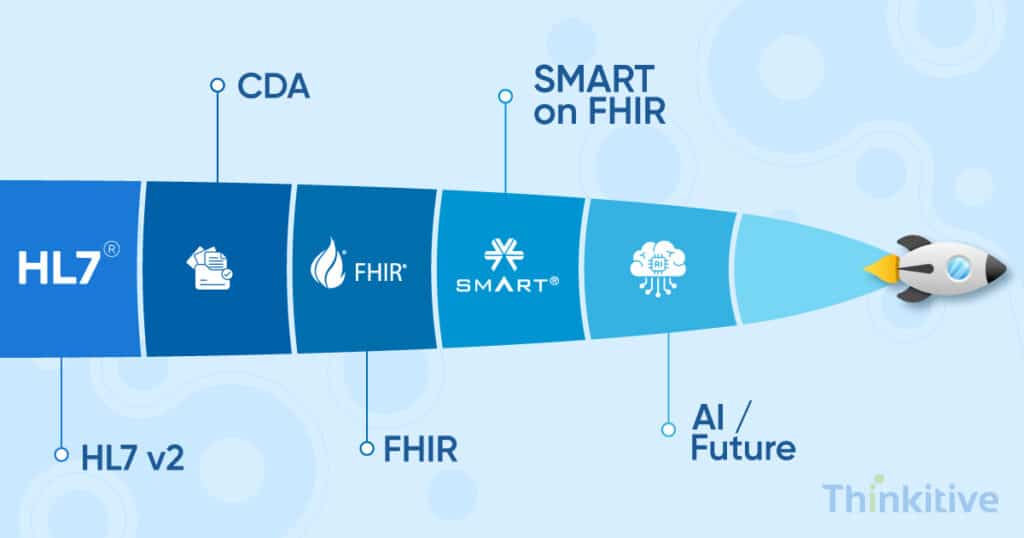
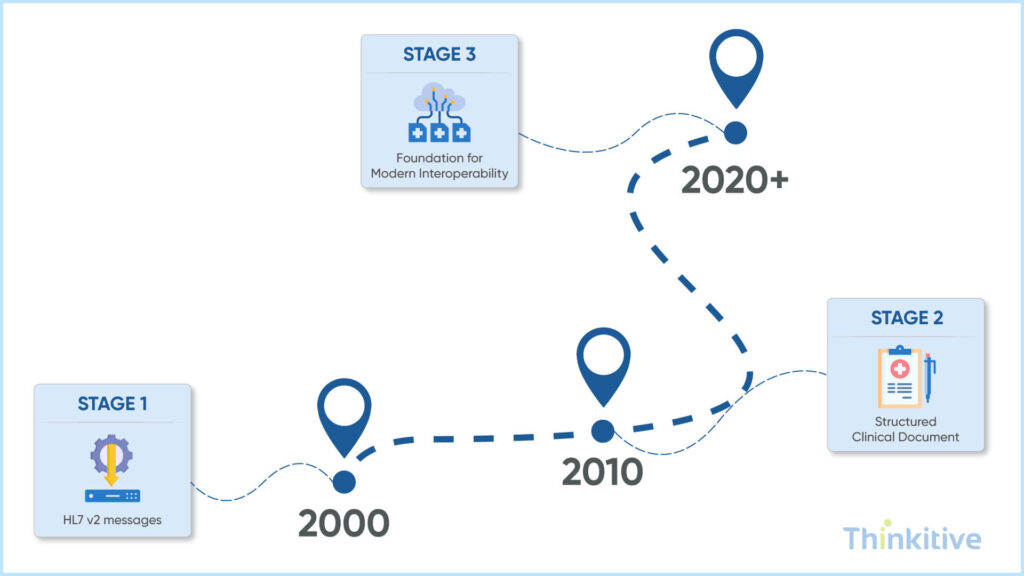
Legacy Standards: HL7 v2 & CDA
Healthcare interoperability standards have evolved over the years, and still, HL7 and FHIR standards dominate the landscape. Interesting APIs and FHIR have been some of the most recent advancements; however, the healthcare landscape is still dominated by legacy standards.
You see, more than 90-95% of the US healthcare organizations still use the HL7 v2 standard for critical data exchange. Some of the most HL7 v2 message types are:
- ADT (Admission, Discharge, Transfer) is used for patient demographics and encounters.
- ORM (Order Message) is used for labs and imaging procedures.
- ORU (Observation Result) is used for lab results and clinical observations.
The reason why HL7 v2 works is that it is lightweight and event-driven. Furthermore, given their flexible nature, they can easily integrate with diverse systems and are supported by almost all systems.
CDA & C-CDA: Structured Clinical Documents
Over the course of time, it was realized that healthcare needed more structured and shareable clinical summaries. This is when HL7 International introduced CDA – Clinical Document Architecture.
This is basically an XML-based document standard that is designed to represent discharge summaries, progress notes, and continuity of care documents. Along with this, a consolidated CDA was also introduced called C-CDA, which standardizes the implementation of CDA and has been widely used for care transitions and patient summaries.
Why Do Legacy Standards Dominate?
Legacy standards still dominate the healthcare system despite better alternatives because they are deeply embedded in healthcare systems. Some of the most prominent reasons are:
- Massive user base
- Higher switching cost
- Vendor dependencies
- Operational reliability
The Role of Regulatory Drivers in Meaningful Use & Document Standardization
The widespread adoption of CDA and HL7 v2 standards was accelerated by regulatory programs like Meaningful Use. These regulatory drivers also promoted the use of certified EHR technology, structured clinical document exchange via C-CDA, and standardized patient summaries during transition of care.
This created a compliance-driven push towards structured interoperability, even though it did not fully allow real-time sharing.
Limitation in Modern Interoperability
While these legacy standards have been the foundation for interoperability, in today’s digital healthcare landscape, they are simply not capable of meeting the rising demands. Some of the key limitations are:
- Lack of true standardization, especially with HL7 v2, which was highly customizable and implemented inconsistently.
- While the world is moving towards API-driven sharing, these standards did not provide native support for RESTful services, which made them difficult to integrate with modern apps.
- These interoperability standards were too document-centric and were not suitable for granular or real-time data access.
- Due to point-to-point integration, scaling became a challenge.
- Last but not least, they provided limited support for patient-facing apps and AI tools.
While HL7 v2 and CDA laid the groundwork for interoperability, their limitations in flexibility, scalability, and real-time accessibility of data have given rise to newer standards such as FHIR. These standards were designed for modern systems that flourished in the API-first healthcare ecosystem.
Modern vs Traditional vs Hybrid: Which EHR Integration Approach Should to Choose –
Get Free ConsultationModern Integration: FHIR & API-Based Ecosystems
The driving factor that changed the landscape of modern-day interoperability is API-driven healthcare powered by FHIR. The advantage that FHIR brought to healthcare was that it enabled real-time, granular, and developer-friendly data exchange. Whereas HL7 v2 focused on events and documents.
HL7 vs FHIR: A High-Level Shift
The difference between these two standards is not just technical but architectural. The table below will make things clear for you:
| Aspect | HL7 v2 / CDA | FHIR |
| Integration Style | Message / Document-based | API-based (REST) |
| Data Access | Batch / Event-driven | Real-time, on-demand |
| Flexibility | Highly customized | Standardized resources |
| Developer Experience | Complex | Modern, web-friendly |
| Scalability | Interface-heavy | API ecosystem |
FHIR Resource Model & REST APIs
FHIR is a resource-based modern web standard that functions by building modular blocks based on patient, observation, encounter, and medication. Along with that, it uses an API to retrieve, create, or update data.
With this integration, across-systems integration becomes easier, the development cycle becomes faster, and consistent data structures can be ensured.
Role in Mobile Apps, Cloud & Real-Time Systems
FHIR has been the foundation for modern digital health experiences. For instance, for mobile apps, it has formed the bedrock for patient portals, remote monitoring apps, and wearable integrations.
On the other hand, for cloud platforms, it enables scalable data storage, makes their microservices interoperable, and allows multi-tenant healthcare platforms. Furthermore, for real-time systems, it allows, for instance, access to patient data, follows event-driven care coordination, and clinical decision support can be provided.
A major catalyst in promoting FIR adoption in healthcare practices has been the 21st Century Cures Act.
SMART on FHIR & the App Ecosystem
The latest advancements in healthcare interoperability have been SMART-on-FHIR, and for good reasons. You see, it enabled healthcare applications to be used as plug-and-play applications.
Being built on FHIR, it uses standardized authentication (OAuth2.0) and provides secure access to EHR data, and provides an app ecosystem that is similar to an app store. With the help of this, many providers have implemented clinical decision support tools, improved patient engagement on applications, and even used them for AI-driven diagnostic assistants.
Frameworks & Real-World Implementation
Till now, you have read or learned about standards, which define how the data should be structured and exchanged. However, in a real-world healthcare environment, that’s just one part of the story.
These standards need a framework to operationalize these standards; in simple words, these frameworks define how these systems work together in clinical workflows.
The Bridge: From Standards to Implementation
Look at these frameworks as the bridge.
Now, where standards ensure consistency, frameworks define the workflow, system roles and responsibilities, and data exchange sequences. Without a framework, even if you standardize your data, it will fail to integrate into disparate systems smoothly.
While talking about framework, you should know about Integrating the Healthcare Enterprise, aka IHE profiles, which makes interoperability actionable. Some of the key IHE profiles are:
- XDS (Cross-Enterprise Document Sharing): Enables the sharing of clinical documents across organizations.
- PIX (Patient Identifier Cross-Referencing): Matches patient identities across multiple systems.
- PDQ (Patient Demographics Query): Allows systems to query patient demographics data.
The simple work of these IHE profiles is that they ensure that systems not only speak the same language but also follow the same workflow rules.
Along with IHE profiles, you must also be aware of DICOM—Digital Imaging & Communications in Medicine—which is used for imaging interoperability. Look at it as a standard for medical imaging, image storage and transmission, and integration with PACS.
This is important because it ensures imaging data is shared across systems such as radiology systems, hospitals, specialists, etc.
Bridging Standards to Real-World Workflows
In a real-world scenario, healthcare interoperability works as a layered ecosystem that uses all the aspects we discussed above. For instance:
- HL7 v2 or FHIR standards are used for data exchange
- SNOMED, LOINC, and RxNorm are used to retain semantic meaning
- IHE profiles for workflow coordination
- DICOM for imaging interoperability
In this way, all these aspects together enable end-to-end clinical workflows, breaking the loop for isolated data transfers.
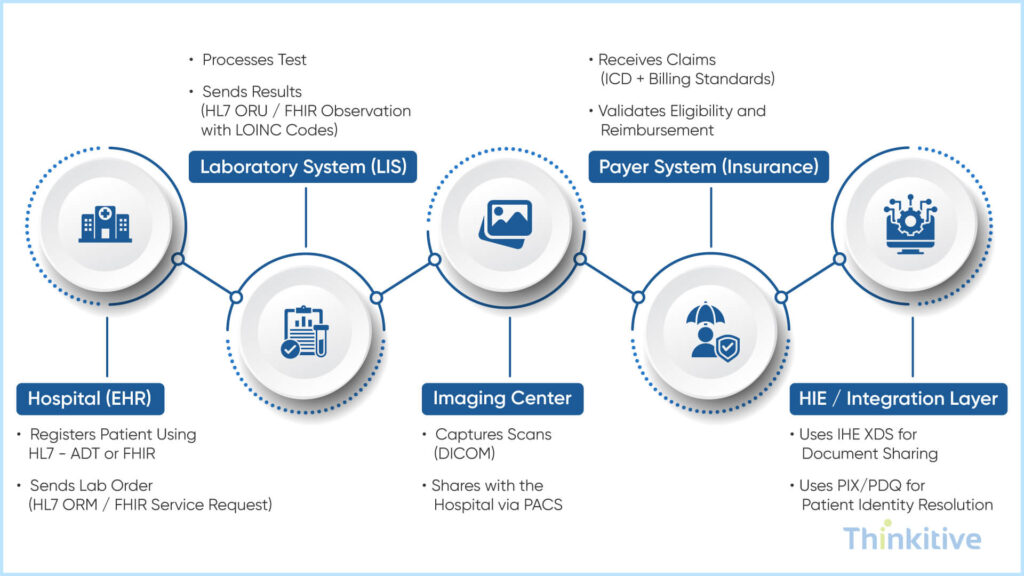
Real-World Example of Multi-System Integration
Let’s look at a typical example of how a connected healthcare ecosystem works. For this, let’s see patient care aspects across multiple systems.
Hospital (EHR)
- Registers patient using HL7 – ADT or FHIR
- Sends lab order (HL7 ORM / FHIR ServiceRequest)
Laboratory System (LIS)
- Processes test
- Sends results (HL7 ORU / FHIR Observation with LOINC codes)
Imaging Center
- Captures scans (DICOM)
- Shares with the hospital via PACS
Payer System (Insurance)
- Receives claims (ICD + billing standards)
- Validates eligibility and reimbursement
HIE / Integration Layer
- Uses IHE XDS for document sharing
- Uses PIX/PDQ for patient identity resolution
The outcome of this is that data flows seamlessly across systems. Along with that, the chances of record duplication and delays are reduced, if not eliminated.
Choosing the Right Electronic Health Record Standards
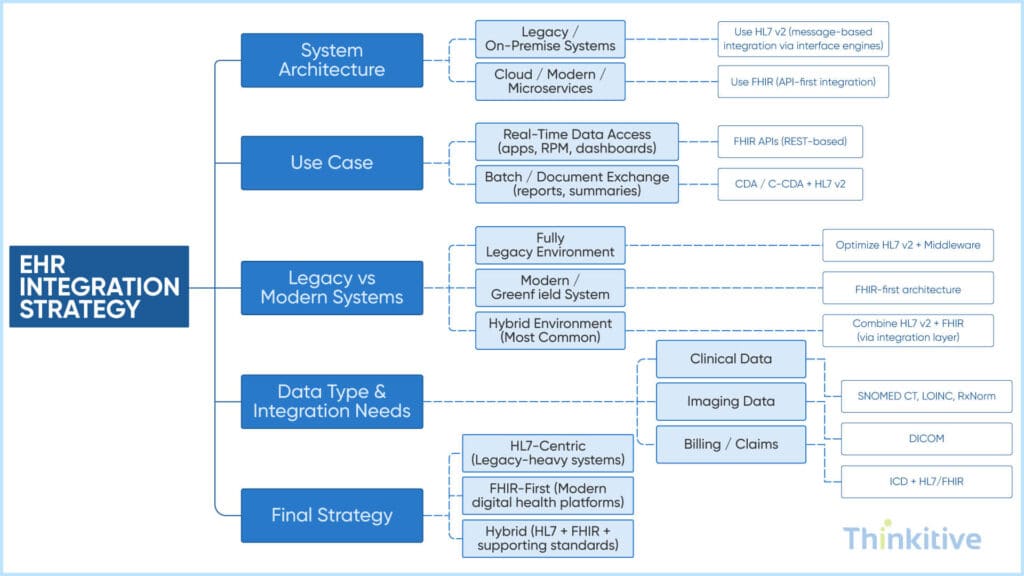
While making this decision, choose the standards based on system architecture. For instance, if you are using monolithic architecture, then HL7 v2 is recommended for legacy systems. On the other hand, if it is microservices, the FHIR or IHE profiles are suggested. It is important because architecture determines whether you need event-based messaging or API-driven interoperability.
Along with architecture, make decisions on the basis of your use cases. If you need standards for real-time access, then FHIR is suggested. However, if you are looking for a scheduled data exchange, then HL7 v2 or CDA is recommended. This is to ensure the system supports timely clinical decision-making.
This is just one example, and such intricacies could be many. Scan this decision tree diagram and make your choices intelligently:
The standards you choose today decide how your system functions tomorrow. That is why the standards should always be chosen in the near future and in some cases in the distant future.
And the best way to do that is to align it with the interoperability requirements and where it is heading. Also, read this definitive guide for making your EHR system a part of the connected healthcare ecosystem – EHR Interoperability: The Definitive Guide to Connected Healthcare Systems.
The Future of Healthcare Integration Standards
So, judging by the tilting sails in the healthcare integration standards evolving landscape, today integration has moved beyond exchanging data. Today, it is becoming more personalized in nature, yet the data flows seamlessly across systems, geographies, and care settings.
You can even argue that it is more about creating a connected, intelligent, and scalable ecosystem. And this evolution in data and how it is being transferred is brought in by the national frameworks, evolving standards like FHIR, and AI-driven automation.
So, here are a few things that you should consider regarding the future of healthcare integration standards.
- TEFCA & National Interoperability Frameworks
TEFCA Stands for Trusted Exchange Framework & Common Agreement. It basically connects multiple Health Information Networks under a unified framework and establishes standardized policies for governance and technical requirements. It can be seen in the majority of countries, such as the United States, the United Kingdom, the European Union, and India.
It is increasing the push for cross-border interoperability standards.
- FHIR Evolution & Bulk Data Exchange
Even after bringing in API based exchange, FHIR continues to evolve, converting into a platform for large-scale and real-time interoperability. In recent years, it has enabled bulk data exports used for population health management, analytics, AI model training, etc. Apart from that, FHIR subscriptions are becoming event-driven to support proactive care workflows, etc.
Emerging Challenges
However, these changes also bring in some challenges that can interrupt or break your interoperability and integrations. On that note, here are a few things that you need to keep in mind:
- Patient-Generated Data: The data generated by a patient is very irregular or unstructured at its finest. First things first, it is generated by apps, wearable devices, RPM devices, etc. And what is irregular about it is its volume, variability, and inconsistent standards, which can be quite hard to validate and connect dots to. In such cases, standardizing the data is the only way to make such data work.
- Cross-System & Global Interoperability: Healthcare systems are spread across the world, and they all vary based on countries, vendors, environments, etc. In such cases, different standards, languages, coding variations, and data privacy laws can be quite hard to come by.
However, you can choose to find a middle ground out of this by using AI-driven automations. You see, it can be used for various things like data mapping, semantic normalization of data, improvement in data quality, and automated workflows. It can reduce manual efforts and accelerate integration timelines, along with accuracy.
HL7 vs FHIR – Which EHR Integration Standard Suits Your Practice –
Get System AssessmentConclusion: Building a Future-Ready Integration Strategy
Even when I started this blog, I did not think it would be this lengthy. Having said that, explaining every point briefly to you is important. So, if you are actively pursuing digital transformation of your practice, let this blog be your guide to choosing the right one.
However, while going, remember this tip: balancing legacy compatibility with modern innovation is important. And this foundation, building a connected healthcare ecosystem, is laid by standards.
On that note, get your requirements aligned, and let’s discuss which standards would be right for you. Book your consultation.
Frequently Asked Questions
EHR integration standards are a set of rules and protocols that enable different healthcare systems—such as EHRs, lab systems, and imaging platforms—to exchange and interpret data consistently.
These healthcare interoperability standards define:
- How data is structured (e.g., HL7, FHIR)
- How it is transmitted (APIs, messaging)
- How it is understood (terminologies like SNOMED, LOINC)
The key difference between HL7 and FHIR standards lies in how they exchange data.
- HL7 (especially v2) → Message-based, event-driven communication
- FHIR → API-based, real-time data access using modern web technologies
In the context of HL7 vs FHIR in healthcare integration:
- HL7 is widely used in legacy systems but requires customization
- FHIR is standardized, flexible, and designed for modern applications
FHIR is considered the future of healthcare interoperability standards because it enables:
- Real-time data exchange via APIs
- Seamless integration with mobile apps and cloud platforms
- Faster development and scalability
- Better support for AI and analytics
Unlike traditional electronic health record standards, FHIR is developer-friendly and modular, making it ideal for modern healthcare ecosystems.
The most common EHR integration standards and protocols include:
- HL7 v2 / HL7 v3 → Messaging standards for system communication
- FHIR → API-based interoperability
- CDA / C-CDA → Document exchange standards
- SNOMED CT, LOINC, RxNorm, ICD → Healthcare data standards for clinical meaning
- DICOM → Imaging interoperability
Healthcare data standards like SNOMED CT and LOINC ensure that clinical data has consistent meaning across systems.
- SNOMED CT → Standardizes clinical concepts (conditions, procedures)
- LOINC → Standardizes lab tests and observations
This improves interoperability by:
- Reducing ambiguity in clinical data
- Enabling accurate data exchange and analysis
- Supporting AI and decision support systems
The 21st Century Cures Act plays a critical role in advancing EHR integration standards by:
- Mandating the use of open APIs (FHIR-based)
- Preventing information blocking
- Promoting patient access to health data
This regulation has accelerated the adoption of modern healthcare interoperability standards, making FHIR a requirement rather than an option in many healthcare systems.
Choosing the right electronic health record standards depends on several factors:
- System architecture (legacy vs modern)
- Use case (real-time vs batch exchange)
- Integration scope (internal vs cross-organization)
- Regulatory requirements
Most organizations adopt a hybrid approach, combining:
- HL7 for legacy systems
- FHIR for modern APIs
- Terminology standards for data consistency
Yes, and in fact, most healthcare systems rely on multiple healthcare interoperability standards working together.
A typical setup may include:
- HL7 for messaging
- FHIR for APIs
- CDA for documents
- SNOMED and LOINC for semantics
- DICOM for imaging




