Introduction to HL7 Standards for Healthcare Data Exchange

Although the healthcare industry is producing 30% of the global data volume, according to the report by RBC Capital Markets, utilizing it all is not easy. The reason? Fragmentation of systems.
The data is not connected, and as per the report by the World Economic Forum, only 3% is used, and the rest, 97% data, just sits in the system. If all the data is leveraged properly, it can easily change how patients are treated, with care plan personalization, improving patient outcomes.
However, the main challenge is that there are multiple sources of data, from medical devices and wearables to patient reports and EHR systems. Without a standardized format, bringing everything together seamlessly is not so simple.
This is where HL7 (Health Level Seven) comes in. Developed in the 1980s as an attempt to make data exchange easier, today it has become the foundation for seamless integration of healthcare systems. It was the first healthcare messaging standard that was successful in standardized data exchange.
But that is only the first step, because it then evolved into HL7 2.x and HL7 v3 to finally what we see today, HL7 FHIR. If you are going to integrate your systems, then knowing HL7 basics is non-negotiable to make the custom EHR integration seamless and successful.
This blog is your guide to HL7 introduction and how HL7 data exchange standards revolutionize healthcare data exchange. We will look into medical data protocols and what makes HL7 v2.x the most adopted version.
So, let’s get started without further ado and understand the basics of HL7.
What is HL7? Understanding the Basics
As mentioned before, HL7 was created in the 1980s. However, this version of the HL7 was developed at the University of California, San Francisco (UCSF) Medical Center. After this, the formal organization was created almost a decade later in 1987, to standardize healthcare data exchange with Don Simborg and some other leaders as founders.
Later, in the 1990s, it became more developed with HL7 v1 and HL7 v2 versions. One more thing that happened is that it was accredited as an ANSI (American National Standards Institute) non-profit organization.
Additionally, level seven in HL7 refers to the seventh layer of the ISO OSI (Open Systems Interconnection) model, known as the Application Layer. This emphasizes HL7’s focus on application-layer protocols for healthcare data interoperability.
Moreover, the main mission of Health Level Seven (HL7) is to connect all disparate systems, such as labs, pharmacies, and EHRs. These healthcare messaging standards enable the systems to speak the same language and exchange all the healthcare data seamlessly.
HL7 occupies a unique and critical role in the healthcare interoperability ecosystem. It maintains the same data exchange capabilities with DICOM, NCPDP, and X12 standards. This standard also specializes in clinical and administrative data exchange protocols and messaging standards.
In short, HL7 has become a cornerstone in healthcare interoperability, and without understanding and adopting it, seamless system integration is next to impossible.
HL7 Standards Roadmap: From HL7 to FHIR
Download nowEvolution of HL7 Standards: From v2 to FHIR
When the HL7 standard was first introduced in the 1980s, it was a basic format for exchanging data from organization to organization. But now it has become the means to seamless interoperability and integration. It has evolved to match the needs and technologies of each era. Let’s take a look at how things changed over the years:
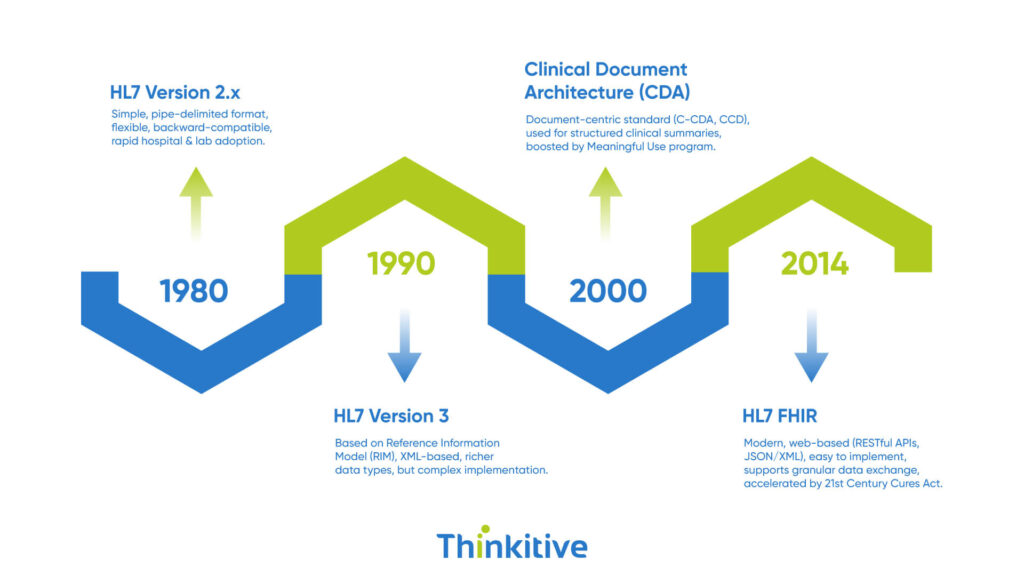
- HL7 Version 2.x: This version, which emerged in the late 1980s, was the most adopted version of the HL7 standard. It was made simple yet effective with its pipe-delimited messaging format. Another reason for its wide acceptance was its flexible implementation that allowed rapid adoption across hospitals and labs. The best thing about this version was its backward compatibility, which allowed it to connect with any new technology easily.
- HL7 Version 3: HL7 v3 was a version that was built to overcome the limitations of HL7 v2. It was based on the Reference Information Model (RIM), a formal, robust semantic framework to ensure precise and consistent data exchange. These messages use XML format, which supports richer data types, improving semantic interoperability. However, it was too complex and much harder to implement, and this led to slow and much lower adoption.
- Clinical Document Architecture (CDA): From v3 came the Clinical Document Architecture (CDA), a document-centric standard designed to exchange structured clinical summaries. CDA, particularly in the form of Consolidated CDA (C-CDA) and Continuity of Care Document (CCD), gained traction during the Meaningful Use Program, enabling consistent sharing of patient records.
- HL7 FHIR (Fast Healthcare Interoperability Resources): This is the latest and modern, web-based approch. It is built on RESTful APIs and familiar web technologies like JSON and XML. FHIR uses a resources-oriented architecture that is easier to implement, test, and scale. It supports granular data exchange and, with the 21st Century Cures Act, is accelerating FHIR adoption.
HL7 v2.x: The Foundation of Healthcare Messaging
Since 1989, the HL7 v2.x has been the backbone of healthcare interoperability, enabling reliable, real-time exchange of patient data between systems. Its delimiter-based, segment-field-component hierarchy makes it lightweight and fast to parse.
This simplicity, combined with extensive optionality, has fueled its global adoption, but also created challenges around inconsistent implementations. Common use cases include patient admission/discharge (ADT), order/result exchange (ORM/ORU), scheduling (SIU), and document sharing (MDM).
Common Message Types & Applications
| Message Type | Purpose | Common Segments | Example Use Case |
| ADT | Patient demographics & visit info | MSH, PID, PV1 | Admit or discharge a patient |
| ORM / ORU | Orders & results | MSH, PID, OBR, OBX | Lab test order & results |
| SIU | Scheduling | MSH, SCH, PID | Book a surgical procedure |
| MDM | Document management | MSH, PID, TXA | Share discharge summaries |
Key Segments & Roles
| Segment | Role | Key Fields |
| MSH | Message header | Sending app, date/time, message type |
| PID | Patient identity | MRN, name, DOB, sex |
Sample HL7 v2 ADT Message
MSH|^~\&|ADT_SYS|HOSPITAL|EHR_SYS|HOSPITAL|202508121000||ADT^A01|123456|P|2.5
PID|||12345^^^HOSPITAL||DOE^JOHN||19800101|M
HL7 Data Exchange Patterns & Transport Protocols

The efficiency of the HL7 depends not only on the message format but also on the way messages are exchanged and transported, meaning the medical data protocols. Understanding these patterns is essential for building reliable, secure, and compliant healthcare integration.
1. Message Exchange Paradigms
- Unsolicited Updates: The Sender transmits data without a request. For example, lab systems send results immediately after compilation.
- Query/Response: Receiver requests specific data, and sender replies with the relevant message.
- Broadcast: Single message sent to multiple recipients simultaneously, often via an integration engine.
- Point-to-Point: Direct connection between two systems for targeted delivery.
- Batch Processing: Groups of messages are transmitted at fixed intervals for efficiency.
- Real-Time Exchange: Immediate message transmission for time-sensitive workflows like ADT events.
2. Transport Protocols & Reliability
- MLLP (Minimal Lower Layer Protocol): The most common transport for HL7 v2, summarizes messages over TCP/IP connections.
- Web Services & HTTP-based Options: Increasingly used with HL7 FHIR and modern integrations for increased interoperability and flexibility with data formats as well as languages.
- Acknowledgement (ACKs):
- Commit ACK: Confirm message receipt.
- Application ACK: Confirms successful processing.
- Error Handling: Use error codes for diagnostics; implement retry logic and queuing to prevent data loss during outages.
3. Security & Compliance
- Transport Layer Security (TLS): Encrypts data in transit to meet HIPAA requirements.
- Authentication & Authorization: Ensures only trusted systems exchange HL7 data.
- Audit Logging: Tracks message access and modifications for compliance and troubleshooting.
By combining the right exchange pattern, transport method, and security safeguards, healthcare organizations can achieve reliable, standards-compliant HL7 messaging.
ls Get the HL7 Implementer’s Kit: Scenarios, Messages & Validation Tools Inside
Download NowPractical HL7 Implementation Considerations
Successful HL7 implementation is more than just sending messages in a standardized format; it’s about ensuring they work reliably in real-world healthcare environments. Every decision, from the choice of interface engine to the way messages align with operational workflows, impacts interoperability, compliance, and clinical efficiency.
Another important thing is that HL7 workflows must fit into an organization’s clinical and operational processes. Event-driven architecture can trigger downstream processes automatically, while orchestration tools can coordinate multi-step workflows that go beyond simple message passing.
Also, testing is crucial in both isolated and through formal certification programs, ensuring a smooth go-live and long-term reliability. Here are the key implementation considerations:
| Category | Key Points | Example Tools/Approaches |
| Interface Engines | Centralize routing, transformation, and monitoring | Mirth Connect, Rhapsody, Corepoint |
| Validation | Syntax vs. semantic checks | HL7 Inspector, NIST Validator |
| Data Mapping | Terminology alignment, type conversion | SNOMED-LOINC mapping, custom scripts |
| Workflow Integration | Event-driven triggers, orchestration | BPM tools, middleware |
| Testing & Certification | Conformance checks, pre-go-live testing | IHE testing tools, vendor programs |
Conclusion
In a nutshell, HL7 is the crucial connecting factor in healthcare interoperability. If a healthcare organization wants to integrate labs, pharmacies, and EHRs seamlessly, then HL7 standards become non-negotiable; despite the new standards like FHIR, understanding HL7 basics remains essential.
So, if you are thinking about integrating your systems, then having a vendor that knows the ins and outs of the HL7 makes the process much easier. Thinkitive can help you, as we have helped many others. Click here and let’s get your integration up and running.
Frequently Asked Questions
HL7 stands for Health Level Seven, a set of international standards that help healthcare systems talk to each other. It ensures patient data moves smoothly, accurately, and securely between hospitals, clinics, labs, and other care providers.
HL7 v2 is lightweight, proven, and great for high-volume, real-time messaging between legacy systems. FHIR is modern, API-friendly, and ideal for app integration, patient access, and flexible data exchange in today’s connected healthcare ecosystem.
In most healthcare settings, HL7 messages like ADT (patient admissions/discharges), ORM/ORU (orders and results), SIU (scheduling), and MDM (document management) handle the bulk of day-to-day data exchange, keeping clinical and administrative workflows connected.
Interfaces act like translators and traffic controllers for HL7 messages. They route data between systems, convert formats when needed, validate structure, and keep everything flowing smoothly so different healthcare applications can talk without miscommunication.
Implementing HL7 interfaces takes technical know-how and healthcare insights skills in HL7 standards, data mapping, interface engine configuration, and a solid understanding of clinical workflows to ensure the tech fits real-world care.
HL7 keeps healthcare systems talking to each other, so patient information flows seamlessly between labs, clinics, and hospitals. This means fewer delays, fewer errors, and more informed decisions, ultimately helping care teams focus on treating patients instead of chasing data.
The toughest parts of implementing HL7 interfaces are dealing with inconsistent message formats, complex data mapping, and ensuring workflows fit clinical reality—all while keeping systems secure, compliant, and relaying to each other.
Regulatory programs like Meaningful Use and the 21st Century Cures Act push healthcare providers to share data more seamlessly. They’ve accelerated the adoption of HL7 standards—especially FHIR—by making standardized, interoperable data exchange a legal and financial necessity.
HL7, DICOM, and NCPDP each tackle different parts of healthcare data—HL7 handles clinical and administrative information, DICOM manages medical images, and NCPDP covers pharmacy transactions. Together, they create a complete, interoperable healthcare data ecosystem.
Healthcare organizations should start by assessing current integrations, mapping data models, and training teams on FHIR’s API-first approach. A phased migration with pilots, strong governance, and vendor collaboration helps ensure a smooth, low-risk transition.




